 Maternal mortality can seem like a throwback to the Victorian era, a bygone relic of a time before modern medical technology turned childbirth from a dicey, high-stakes gamble into an anodyne rite of passage. I must admit that until recently, I, a practicing pediatrician, agreed with this view – despite the fact that my great-grandmother died in childbirth and my grandmother nearly suffered the same fate. But statistics on childbirth and the local case of a 2014 death at Naval Hospital Bremerton, back in the news just this week, remind us of the risks that still exist to a high degree in our developed world.
Maternal mortality can seem like a throwback to the Victorian era, a bygone relic of a time before modern medical technology turned childbirth from a dicey, high-stakes gamble into an anodyne rite of passage. I must admit that until recently, I, a practicing pediatrician, agreed with this view – despite the fact that my great-grandmother died in childbirth and my grandmother nearly suffered the same fate. But statistics on childbirth and the local case of a 2014 death at Naval Hospital Bremerton, back in the news just this week, remind us of the risks that still exist to a high degree in our developed world.
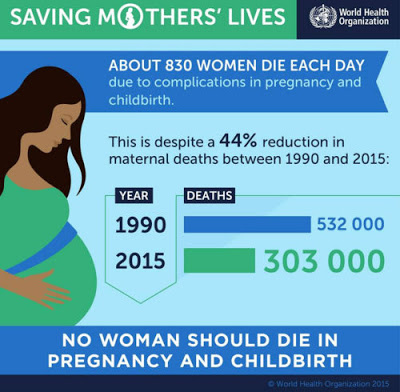
According to the World Health Organization, the global maternal mortality rate has fallen by 44 percent in since 1990, with 157 of 183 countries tracked by the organization experiencing a decrease between 2000 and 2015. The United States, however, was not among those 157 countries.
During the same period, the U.S. maternal mortality more than doubled, skyrocketing from 9.8 to 21.5 maternal deaths per 100,000 live births. That’s six times higher than most Scandinavian countries and three times higher than Canada and the United Kingdom. In the U.S., around 700-900 women die and another 65,000 experience life-threatening complications during or after childbirth. By any standard, the U.S. has the worst performance on this crucial measure of any country in the developed world.
And while complications from pregnancy and childbirth can, of course, strike women of all backgrounds, maternal mortality in the U.S. afflicts certain demographics –African Americans, low-income women and those living in rural areas– much more than others. According to the Centers for Disease Control, the maternal mortality rate is three times higher for African American women than white women. (40.0 vs. 12.4 deaths per 100,000 live births in 2011-2014.)
To make matters worse, research done by the CDC Foundation determined up to 60% of these maternal deaths were preventable.
These stats got me thinking: Seeing that maternal mortality clearly remains a serious problem, why are we taking a head-buried-in-the-sand approach? (The most recent nationwide maternal mortality statistics date from 2007.) And how can childbirth in the U.S. become equally as safe as it is in Libya or Vietnam?
Since 2006, the state of California has been working with Stanford University School of Medicine to buck the status quo, by starting the California Maternal Quality Care Collaborative (CMQCC), aimed at developing best practices to reduce maternal mortality. The medical director at CMQCC, Elliott Main, formed a review board made up of concerned doctors, nurses, midwives, and hospital administrators to analyze root causes of mortality and propose solutions. Through their work, it quickly became apparent that hemorrhage and preeclampsia were the most common preventable causes of maternal death.
While hemorrhaging is associated with such risk factors as delivering twins or having multiple pregnancies, as many as one-third of mothers don’t fit into a risk profile. This means that a life-threatening hemorrhage – which can be lethal in under five minutes– often comes on suddenly making time, of the essence. The maternal mortality review board found that obstetric teams were often unprepared to deal with unexpected hemorrhaging and wasted precious time searching for the drugs and supplies needed to staunch bleeding.
Hopsitals have had “code carts” for decades – wheeled contraptions stocked with basic equipment necessary to resuscitate patients – so why, the mortality review team reasoned, don’t obstetric units have “hemorrhage carts” to keep all the emergency supplies in one easy-to-reach place?
The CMQCC team also took umbrage with the tried and true practice of eyeballing maternal blood loss. There are better, more objective ways of measuring real blood loss. They recommended that obstetric teams weigh the pads and sponges they use to collect blood before and after they are soaked to quantify the exact volume of blood loss and therefore replace losses when necessary.
Another top maternal killer, a condition called preeclampsia, is highly treatable, if caught early and treated aggressively. However, it’s been shown that in fatal cases, healthcare providers fail to do either. In 2014, CMQCC developed a “preeclampsia toolkit” calling for more careful monitoring of blood pressure and swift administration of magnesium sulfate and anti-hypertensive medications when vital signs indicate abnormal blood pressure readings.
While data evaluating effectiveness of CMQCC’s approach has yet to be published, among the 126 hospitals taking part in the group’s maternal hemorrhage and preeclampsia projects, maternal morbidity fell by 20.8 percent between 2014 – 2016. And overall, their efforts are credited with helping the state of California reduce its maternal mortality rate by 55 percent from 2006-2013. The state’s rate dropped from 16.9 to 7.3 per 100,000, even as the U.S. maternal mortality rose from 13.3 to 22.0 per 100,000 during the same period.
Though, in Washington State, our maternal mortality ratio has held steady at 9.0 per 100,000 births for years, we too stand to learn from California’s example. Childbirth is no party. It can be one of the riskiest endeavors women face in their lifetime. We must mobilize our health providers, policy-makers, and communities to do better. With increased awareness of maternal mortality– and tangible, targeted actions to ensure pregnant women receive the highest quality care– many fatal and near-fatal outcomes can be avoided.