As policy experts cling to pay-for-performance (P4P) as an indicator of healthcare “quality” and shy away from fee-for-service, childhood immunization rates are being utilized as a benchmark. At first glance, vaccinating children on time seems like a reasonable method to gauge how well a primary care physician does their job. Unfortunately, the parental vaccine hesitancy trend is gaining in popularity. Studies have shown when pediatricians are specifically trained to counsel parents on the value of immunizations, hesitancy does not change statistically.
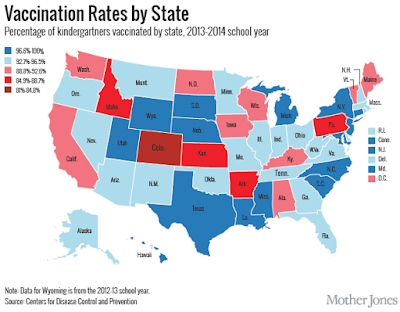
Washington State Law allows vaccine exemptions on the basis of religious, philosophical, or personal reasons; therefore, immunizations rates are considerably lower (85%) compared to states where exemptions rules are tighter. Immunization rates are directly proportional to the narrow scope of state vaccine exemptions laws. Immunization rates are used to “rate” the primary care physician despite the fact we have little influence on the outcome according to scientific studies. Physicians practicing in states with a broad vaccine exemption laws is left with two choices: refuse to see children who are not immunized in accordance with the CDC recommendations or accept “low” quality ratings when caring for children whose parents with beliefs that may differ from our own.
The more willing a physician is to care for those with differing philosophical, religious, and cultural beliefs, the more CMS metrics will discriminate against our open-hearted approach. Reflecting upon my medical school admissions interview, my open heart and mind are some of the reasons for entering medicine in the first place. As I contemplated my tumbling quality indicators by continuing to see children regardless of immunization status, I stumbled upon some ICD-10 code gems:
- Z28.0 – Immunization not carried out because of contraindication
- Z28.01 – Immunization not carried out because of acute illness of patient
- Z28.02 – Immunization not carried out because of chronic illness or condition of patient
- Z28.03 – Immunization not carried out because of immune compromised state of patient
- Z28.04 – Immunization not carried out because of patient allergy to vaccine or component
- Z28.09 – Immunization not carried out because of other contraindication
- Z28.1 – Immunization not carried out because of patient decision for reasons of belief or group pressure
- Z28.2 – Immunization not carried out because of patient decision for other and unspecified reason
- Z28.20 – Immunization not carried out because of patient decision for unspecified reason
- Z28.21 Immunization not carried out because of patient refusal
- Z28.29 – Immunization not carried out because of patient decision for other reason
- Z28.8 – Immunization not carried out for other reason
- Z28.81 – Immunization not carried out due to patient having had the disease
- Z28.82 – Immunization not carried out because of caregiver refusal
- Z28.89 – Immunization not carried out for other reason
- Z28.9 – Immunization not carried out for unspecified reason
Surprisingly, ICD-10 and the advanced coding technology might have had some unanticipated benefits. If a physician uses vaccine refusal codes appropriately, the patient in question should be removed from the denominator being used to calculate immunization rate for a given clinic or physician.
This allows immunization rates to reflect “quality” while accounting for factors outside the control of the primary care physician. Vaccine exemption laws must be considered confounding variables when using immunization rates as a quality metric; eliminating confounding variables purifies the data set. This is a simple concept, so why are metrics being collected by CMS not controlling for caregiver refusal when it is mandated by law? Accuracy is the point of collecting data in the first place, right? If you believe CMS is interested in accuracy, then I have a bridge somewhere to sell you on the Olympic Peninsula.
ICD-10 codes already allow for regional specificity; a physician in Washington State has codes when a patient is pecked by a chicken (W61.33) or bitten by a cow (W55.21); there is even a code when a one is struck by an Orca Whale (W56.11), an event more likely to occur in Washington than Idaho. If we can code for injuries sustained when our water skis catch on fire (W91.07) after a civilian boat collided with a military watercraft (V94.810) while waterskiing on the Puget Sound near the Naval Undersea Warfare Center Keyport, then we certainly should be capable of controlling for confounders which do not reflect the “quality” of care a physician provides.
Claude Levi-Strauss, once said, “The scientific mind does not so much provide the right answers as ask the right questions.” Immunization rates are clearly NOT an accurate quality indicator. Maybe it is time for policy experts and physicians to question what constitutes the provision of high-quality health care in the first place. Only then, can this country move in the right direction.